
 |
| Thanks to Arnold Dreyblatt for this image |
Lots of vaccine news, some mandate lessons from Italy, more on those pesky CDC guidelines, plus some Omicron miscellany.
Treatment and mitigation

RegenCov: I was surprised that the Phase 3 trial of Regeneron’s monoclonal antibody treatment, from when early variants of SARS-CoV-2 were dominant, was published only last month. The product does work against the Delta variant – though likely not against Omicron.
RegenCov and Lilly: I mentioned in my last post that the federal government stopped distributing both these monoclonal antibody products to the states, based on fallacious figures from the CDC. Now they have resumed distribution, but are getting flak for it because of the Omicron story. This criticism is misguided, both because there is still a lot of Delta around in the US and because Omicron is less likely to send people to the hospital.
Masking: I was slow to accept that face masks would help curb transmission of the coronavirus, but now I’m a convert. If I hadn’t been, a recent comparison of countries with and without mask mandates in the spring of 2020 would have convinced me. The difference in daily per capita COVID-19 mortality was huge: 288.54 per million in countries without face mask policies, 48.40 in countries with face mask policies. The researchers picked a period when all 44 study countries had restricted movements and gatherings, and were able to take other mitigation measures into account. The US and Canada were excluded because the rules varied so much from state to state. Italy, incidentally, is now requiring KN95 masks inside both public transport and cultural events.
Keeping safe: I’ve examined and tested many calculators intended to help people gauge how risky a given activity is, and the best I’ve seen is this one.
Ivermectin: The ivermectin-mongering physician Paul Marik, whose chief paper was withdrawn after his hospital revealed he’d faked the statistics, has prudently chosen to resign from his teaching position at the East Virginia Medical School before getting the boot. So now he’ll have more time for spreading pandemic lies and conspiracy theories.
Weed? Research from the Linus Pauling Institute (check out what the institute says about vitamin C) made a huge splash under headlines such as Bloomberg’s “Cannabis Compounds Prevented Covid Infection in Laboratory Study.” Actually those cannabinoids – which included CBD but not THC – did nothing of the sort. They merely blocked SARS-CoV-2 from entering cells in a testtube, in a study so far behind the times that the its examples of “the most concerning and widespread” variants are Alpha and Beta. Know what other drugs do the same thing? Heparin,umifenovir, ivermectin and hydroxychloroquine, all of which flopped as antivirals in human bodies.
Azithromycin (Zitromax, Z-pak): Despite having been proven a year ago to have no value in treating COVID-19 either inside or outside the hospital, this antibiotic is being prescribed so much by ignorant Italian doctors that pharmacies have run out. Unfortunately only a few Italian science writers have done their homework.
Vaccine news

Sinovac’s Coronavac: Already the least effective vaccine around, albeit widely used worldwide. Now a lab study says it’s likely to be completely useless against the Omicron variant.
Boosteritis: Pfizer boosters have now been shown to reduce infection rates by over 90% as compared with “complete” vaccination, and to be particularly effective in young people ages 16-29. Israel is now moving on to 4th doses for healthcare workers, people over 60, and the immunosuppressed. Chile is following suit, though only in the immunocompromised. They should probably broaden eligibility, given their dependence on Sinovac.
Johnson & Johnson: Preliminary results from a study among South African health workers suggest that a two-dose regimen – with a booster 6-9 months after the first shot – provides 85% protection against hospitalization due to the Omicron variant. That looks at first glance about as good as Pfizer. But the extremely high proportion of South Africans who have had COVID-19 (about 70%), means that population has an additional source of immunity, so this study can’t be generalized elsewhere. The follow-up period was also very brief, and the efficacy of the J&J vaccine tends to wear off fast.
Corbevax: I got the spelling wrong last time but not the lack of evidence in its favor. Let’s root for high efficacy, especially since the Texas group have deliberately and generously created a cheap and easy vaccine aimed at the developing world (it’s even vegan and halal!). For one millisecond I thought there actually had been Phase 3 trials, before discovering that the term was being misused: the trials they’re calling Phase 3 were actually only Phase 2, showing the vaccine was “safe, well-tolerated, and immunogenic.” Real Phase 3 trials, looking at real-world efficacy among tens of thousands of volunteers, don’t even seem in the works, just one using Corbevax as a booster dose.
Novavax: The United States/Mexico Phase 3 trial has now been published, with nothing new since we first saw the preprint of the manuscript: topline efficacy of 90%, long before Delta appeared on the scene. The company says the antibodies their vaccine elicits should knock out Omicron, let’s hope.
CanSino: Hadn’t heard from them for a long time, but now a Phase 3 trial has shown 57.5% efficacy against symptomatic COVID-19 and 90% efficacy against severe disease, after a single dose. But it worked less well in women and in people over 60, and protection began to wane quickly. Though that topline efficacy is less than other viral vector vaccines, Johnson & Johnson and AstraZeneca, CanSino’s could be useful in the developing world given easy storage in the fridge.
Pfizer vs. Moderna: A case-control study among American healthcare personnel, unfortunately pre-Delta, proves once again that Moderna rules the roost. It was more effective than Pfizer both after a single dose (89% vs. 78%) and after a complete two-dose course (96% vs. 89%). Effectiveness decreased slightly overall by 13-14 weeks, but too few subjects had received Moderna to be able to detect differences.
AstraZeneca: The sole properly-performed Phase 3 trial, the one conducted mostly in the United States, has now been published, 10 months after the company suffered the humiliation of being publically reprimanded by the US Food and Drug Administration for fudging its data. Overall efficacy was 74%, considerably less than the 79-80% that had been announced in the company’s original press release, though better than the 64% in AstraZeneca’s crummy original trials. This vaccine has been abandoned in Europe and even (almost entirely) in its native UK due to clotting complications, and will certainly never be used in the US, but it can still be valuable in the developing world. This is yet another study that predated Delta… Against Omicron the best AstraZeneca can claim is that a 3-dose series produced as many neutralizing antibodies as 2 doses of Pfizer. Since a 2-dose course of Pfizer gives only 33% protection in the real world, that’s really nothing to brag about.
Universal vaccines: Articles last spring in Science and The Atlantic described a variety of approaches researchers are taking to create a vaccine that might knock out current and even future variants. One, from biologist Pamela Bjorkman in California, cobbling together spike protein fragments from several coronaviruses, stimulated antibody production in miceeven against some coronaviruses not included in the vaccine. Another approach is illustrated at the top. A recent think piece by Anthony Fauci and colleagues breathed new life into the subject by brilliantly setting out the necessary and desirable properties of such a vaccine. But they had little to say about how to achieve it.
Do vaccines make infected people less contagious? A British study says people fully vaccinated with Pfizer are half as likely to transmit infection as those who are unvaccinated, though that advantage falls markedly over 14 weeks. AstraZeneca’s already paltry edge reaches zero by 12 weeks.
Should COVID-19 survivors get vaccinated? Brazil has investigated, and found additional protection from vaccination over natural immunity that ranges from 39% for Sinovac to 65% for Pfizer, with AstraZeneca and J&J in between. Everybody should get vaccinated.
Myocarditis redux, again: A study by an Israeli insurance company, limited to people 16 and over, puts the risk after the first vaccine dose at about 1 in 10,000 male vaccinees between 16 and 29 years old. Since the incidence is known to be higher after the second dose, this is consistent with the 1 in 6273 after dose 2 for boys 12-18 in a US study based on Vaccine Adverse Event Reporting System reports. The authors of the VAERS study are somewhat dubious, with a slight odor of novax, and a BMJ article has criticised their results. But even tainted messengers can at times bring a correct message, and I fear this is one of those times. The VAERS results are very close to the 1 in 6637 estimated for Israeli boys ages 16-19 in a population-wide analysis. They also jibe with a brand-new UK study that found myocarditis during the 4 weeks after dose 2 in one in 9900 males under 40, a rate 14 times higher than the rate of myocarditis following a positive test for SARS-CoV-2; there were too few adolescent boys to analyze separately. The CDC has acknowledged the complication, “predominantly in male adolescents and young adults,” without providing any statistics of its own.
Omicron: Our best current info comes from the UK’s December 31st government report. A single dose of Pfizer or Moderna lowered the risk of Omicron hospitalization by 52% as compared with unvaccinated controls, 2 doses by 72%, and 3 doses by 88%. Against any symptomatic Omicron, double-dose AstraZeneca was less than 30% effective and by 20 weeks it was totally useless. Two doses of an mRNA vaccine started out around 60% but by 20 weeks barely beat AstraZeneca. A booster dose of Pfizer raised effectiveness to 60%, though by 5 weeks the improvement was already slipping. Moderna did better, as usual, hitting 70-80% protection lasting at least 9 weeks. At this point the only image that gives me any sense of optimism is of Pfizer’s scientists working like mad to develop an Omicron-specific vaccine. If they succeed I’ll be the first on my block to hold out my arm.
Variant watch
 |
| Didier Raoult |
B.1.640.2: Remember Didier Raoult, the French celebrity virologist who caused unmeasurable harm early in the pandemic with fake research that spawned the hydroxychloroquine craze? He’s resurfaced, describing a dozen cases of a new SARS-CoV-2 variant imported from Cameroon. It doesn’t have a Greek letter yet, and may never get one given the lack of concern in WHO circles, but Raoult has immodestly dubbed it IHU after his own workplace, the Institut Hospitalo-Universitaire.
Flurona: Don’t be fooled. This is not a new variant, but one unvaccinated pregnant woman in Israel and a few young people in the US who got infected with two viruses at once, influenza and SARS-CoV-2. Double infections like this do happen, and the patients have all recovered quickly.
Deltacron: Researchers in Cyprus say they’ve found 25 cases of a novel variant, with Omicron-like genetic signatures within a Delta genome. But many experts think they’re being fooled by cross-contamination in the lab.
Staying home in the USA

After widespread shock greeted the CDC announcement of drastically slashed guidelines for quarantine and self-isolation, Anthony Fauci dropped hints that the agency might at least add a testing requirement. But no, they’re sticking to their guns, allowing people back in the community after 5 days without testing, though saying that if for some reason a person “wants to test” it’s permitted. This choice seems to be for the worst possible reason: nobody follows the rules anyway. According to NPR, “studies suggest” that only 25-30% of Americans with COVID-19 actually stay home for 10 days as they are supposed to. Equally embarassing is how expensive and scarse antigen tests are in the US.
And here’s the kicker. Antigen tests are already lousy at detecting Delta, notoriously missing as many as 50% of infections, and they’re turning out to be even worse at picking up Omicron. Some tests are completely unable to detect the new variant. Even those that supposedly work, don’t work well. One scrupulous study studied viral loads and traced contacts on 30 vaccinated and boosted patients with PCR-proven Omicron COVID-19, having them test at home daily with Abbott BinaxNOW and/or Quidel QuickVue. Judging from viral loads, most of them were contagious for 3 or more days before the antigen test became positive, during which time 4 transmitted the infection to other people. Previous reassurances about precisely those tests had come not just from the Quidel and Abbott companies, but also from the FDA. I find this news scary and depressing. It implies that having a negative rapid test doesn’t mean much, whether for protecting your family at gatherings or for getting out of self-isolation. Interestingly, throat or salivary swabs seem better than nasal swabs when it comes to Omicron, unlike earlier viral strains. I wonder whether Quidel and Abbott are the home testing kits soon to be sent by the Biden administration to American families, supposedly free but more likely a pricing nightmare.
As for the supposed science underlying the 5-day limit, the chief research cited by the CDC is a British modeling study estimating that only 31% of Omicron cases are still infectious 5 days after their positive test. HOWEVER. Firstly, 31% is far from zero. Secondly, booster shots are our best bulwark against Omicron, and more than twice as many people have received them per capita in the UK (50%) than in the US (22%). Thirdly, on one informal poll 43% of American Omicron patients still had positive antigen tests more than a week after the first one, and given the tests’ low sensitivity even more were likely still infectious. Italian experts recommend current antigen tests be scrapped for making any important decisions. Better ones must be developed, manufactured, and distributed, fast.
Then there’s the justification CDC chief Rochelle Walensky gave to the Washington Post for not requiring testing. It’s ridiculously off the point: PCR tests “can yield positive results even when the patient is not infectious.” True, but those false positives occur far later than 5 days and, besides, no one’s proposing PCR tests for getting out of quarantine or self-isolation, especially not in the US, where results can take 6 days.
Remember in May when Walensky said vaccinated people could stop wearing masks, on the honor system? Remember when she decided to stop tracking breakthrough infections if they didn’t lead to hospitalization or death? Remember her false reassurance in July: “If you're fully vaccinated, you are protected against severe COVID hospitalization and death and are even protected against the known variants, including the delta variant”?
This woman is just not up to the task.
I hear she’s hired a media consultant to help her messaging (“Rochelle Walensky Is Not Good At This”) But in my opinion the problem is at least as much with the substance as with the spin.
Staying home in Italy

Italy is more pandemic-cautious than the US, but it too is somewhat relaxing quarantine and self-isolation guidelines. A December 31st decree lets close contacts who are boosted, recently vaccinated, or recently recovered skip quarantine. But that’s only if they remain asymptomatic all week, wear a KN95 mask for 10 days, and test negative 5 days after their last exposure. Anyone who’s not fully vaccinated must still quarantine for 10 days, and people who completed their vaccination more than 4 months ago and haven’t been boosted must quarantine for 5 days followed by a negative test. In my opinion the reduced duration is a mistake, because Delta, still the dominant variant in Italy, has a longer incubation period.
Self-isolation of individuals who test positive but have no symptoms has also been reduced, from 10 days to 7, but that’s only if they are boosted or recently vaccinated, and in any case they must do a swab at the end. For everybody else self-isolation remains 10 days, again closing with a negative swab. For what they’re are worth.
The rules are so confusing that even science journalists get them wrong, for example: “Self-isolation only lasts 5 days and if there are no symptoms a negative swab is not required.”
Omicronicles
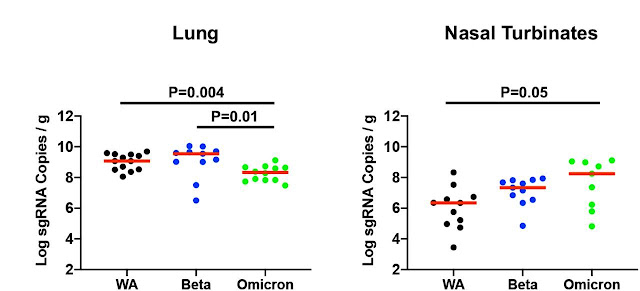 |
| Amount of 3 viral strains growing in hamster tissues |
Might the current American surge peak in mid-January and then fade fast? That’s what some predict, based on the brevity of the Omicron spikes in South Africa and perhaps in the UK. I’ve been skeptical about extrapolate the Omicron experience of either country to the US or Western Europe, because of South Africa’s young population and sky-high previous infection rate, and the UK’s super booster campaign. But there are some hints that the Pollyannas may be right, with wastewater coronavirus levels falling in Boston and cases starting to plateau in New York City. As I too often find myself saying, time will tell.
I’ve previously described a study of surgical specimens that found Omicron to grow well in upper respiratory tissues but poorly in the lung, explaining lower rates of pneumonia. This has been confirmed now in laboratory animals, with the above figure showing viral load in hamster tissues 4 days after inoculation. The figure is on a logarithmic scale, so the differences are larger than they look: compared with the wild strain Omicron grew 74% less in the lung, 90% morein the nose.
Remember that party in an Oslo restaurant where 150 people came down with COVID-19 within days? Investigators now say that one person, who had returned from South Africa several days earlier, infected all of them in a single evening. Wow.
We know previous infection with Delta doesn’t protect against reinfection with Omicron. How about vice-versa? A South African study found that neutralizing antibodies against Delta increased in 13 patients after they had Omicron infections. However: 1) this is a very tiny study; 2) neutralizing antibodies in the lab do not necessarily translate into real-world protection; 3) we cannot generalize from these patients, all previously infected with Delta, to Delta-naïve people; 4) this would be relevant only in countries where the two strains coexist, currently including the US (41.4% of new cases are Delta) and Italy (79%). Given how quickly Omicron has replaced Delta in the UK and several EU countries, cross-immunity may soon be irrelevant. The World Health Organization has made the horrifying predictionthat more than 50% of Europeans will be infected with Omicron over the next 6-8 weeks, with Anthony Fauci extending that to “just about everybody.”
Evidence that Omicron causes milder disease keeps piling up. A study of nearly 600,000 American patients followed over 3 days found that those diagnosed on December 15th-24th, when Omicron was spreading rapidly, were 56% less likely to be hospitalized, 67% less likely to wind up in the ICU, and 84% less likely to need a ventilator, than those – all Delta diagnosed (with Delta) during the previous 18 weeks. And in a UK government report analyzing a million cases between November 22nd and December 26th, half Omicron and half Delta, the risk of hospital admission was two-thirds lower with Omicron.
Mandate sanity Italian style
 |
| Not much distancing at this vaccine hub in Naples |
Researchers have studied how effective “Green Passes” are in promoting vaccination, and the bottom line is “very.” Here’s a concrete Italian example. During the first half of November, when unvaccinated people could still get into a restaurant or a movie theater based on an antigen swab, vaccinations were at a standstill – only 270,000 novaxers went for a first dose. In the second half of November a “Super Green Pass” (no test option) was pre-announced, and 340,000 novaxers repented. In December the rules actually tightened, and between the 1st and the 15th, 490,000 novaxers folded…. Out of 7 million people over 12 unvaccinated on November 1st, nearly 2 million had had a dose by December 31st. Yippie!
The latest Italian decree is in my opinion just what the doctor ordered: a vaccine mandate for everybody over 50. But if someone refuses to comply all they face is a one-off 100 euro fine (about $114). Is this some kind of joke?
Italy’s making life so hard on the unvaccinated – now they can’t even get on a city bus – that one novax acquaintance and her mother are planning to move to the United States.
Italy remains laser-focused on vaccines, which though invaluable won’t have any immediate effect. In the meantime COVID-19 infections are soaring, ICU cases creeping ominously upward, and even the daily death toll triple what it was at the beginning of December. At least everybody here wears masks inside public spaces and they’re testing like mad. But sporting and cultural events are cheek-to-jowl, nobody’s working from home, and young people party like it’s 2019. I say fix all that and impose a curfew. Plus why not add a lockdown for novaxers, with cops doing random checks on the streets flanked by out-of-work young people hired for the occasion? The one Austria instituted in December quickly (but alas briefly) slashed its case numbers by 80%. Drastic, but the only way I see to ward off a real lockdown.
Mandate madness Italian style

COVID-19 vaccination for healthcare workers has been obligatory in Italy since this summer, with thousands of unvaccinated doctors, nurses, and hospital personnel already suspended without pay. More are still being ferreted out, as the professional licensing boards gain access to official vaccination data bases they can cross-tabulate with their membership rolls.
For months the mandate was hailed as essential protection for patients, with nobody made a public peep in opposition. That ended December 19th, when 40 or 50 no-vax physicians screamed their way into a meeting of Rome’s medical organization, shoved their colleagues around, commandeered the mic, and read out a manifesto against being forced to take “experimental” vaccines. I thought that kind of thing only happened in America! But I find it even more shocking that Rome’s medical organization has only suspended a few dozen unvaccinated physicians, when it claims to have evidence that 600 of them are still plying their trade on hospital wards and in General Practitioner offices, 8 months after the mandate and suspension order kicked in.
No comments:
Post a Comment