A wide-ranging post: from convalescent plasma to boosters, American healthcare, CDC guidelines, long COVID, excess mortality, leak vs. leap, and global mishegos.
Treatment and prevention news
 |
| An Italian classroom |
Convalescent plasma (serum): A treatment that rises continually from its ashes. In a new large American study, recent-onset patients who received high-antibody plasma saw their risk of hospitalization slashed in half. Even though most plasma donors had had the Wuhan wild strain, their sera protected against Delta. If donor and recipient strains had matched, the treatment might have done even better. The researchers point out that unlike monoclonal antibody products, convalescent serum contains a broad range of antibodies, adding that plasma sourced locally from recent survivors might be particularly effective.
Ventilation: A study in one Italian region says controlled mechanical ventilation in classrooms can cut kids’ infections by as much as 82.5%, pretty amazing. I need to see more details, because the classroom isn’t where most children get infected. Ventilation systems might be most valuable in adult venues such as theaters and medical conferences.
Lockdowns: A nice piece in The Conversation demonstrates that lockdowns are extremely effective when instituted early, while pointing out that they represent a failure of more gradual policies. Its data should silence the few remaining doubters.
Vitamin D: People with low vitamin D levels have a high risk for severe COVID-19. Yes. There’s even a self-styled meta-analysis claiming that a “Mortality Rate Close to Zero Could Theoretically Be Achieved at 50 ng/mL 25(OH)D3 [a high blood level of vitamin D].” I’ve always been convinced the association was due to confounding: people in poor health have low levels. Now there’s proof. In a gigantic British study, adults with lowish vitamin D levels who were randomized to receive high-dose supplements were if anything more likely to fall ill with COVID-19, be hospitalized, or develop long COVID. These results held even when people randomized to supplements but didn’t take them and people randomized to no supplements took vitamin D outside the study setting were excluded from the analyses.
Ivermectin: The large-scale Brazilian study that put the final nail into its coffin has now been published. But I doubt that will stop ‘mectinmania.
Sotrovimab: Bad news. The only monoclonal antibody product that worked well against the original Omicron variant turns out not to work against BA.2, which has taken over much of the world, so the FDA has stopped shipments to areas of the US where it’s dominant. Next up to the plate is the new arrival, bebtelovimab.
Antivirals: What’s with Italy? Though more than 11,000 doses of Paxlovid touched down by February 3rd, and many more since, only 2,072 patients had been treated as of March 22nd. The less effective Lagrevio (molnupiravir) had gone to more than 4 times as many, and I’m unable to find how many have had infusions of remdesivir. About 384,000 people over 70 were diagnosed with COVID-19 during that time frame, most of whom would have been eligible for antivirals.
Vaccine news
Booster #1: Yet another study, analyzing Pfizer Phase 3 follow-up data during the Delta wave, has confirmed that a third dose heps up effectiveness to well over 90%. But we know it’s less effective against Omicron, and that it doesn’t last long. There is now laboratory evidence that the Moderna booster would be much more effective against Omicron if it contained 100 µg of mRNA instead of 50.
Booster #2: This is what everybody’s asking me about, and I don’t always know what to say. Along with Israel and several European countries, the US is plunging ahead with 4th shots to older people. But their value has still not been definitively demonstrated. An Israeli study of healthcare workers, using age-matched controls, found vaccinated subjects to have only 11-30% fewer infections and 31-43% lower rate of symptomatic COVID-19. Another study, in the general Israeli population, found substantially increased protection against infection, but it had vanished just 8 weeks after the 4th dose; enhanced protection against severe disease lasted at least 6 weeks. Now a third Israeli study, from an insurance company, reports that deaths from COVID-19 were 78% lower for 40 days following a second booster. But before leaping to conclusions, note that this study was not a prospective trial but a retrospective comparison between people who chose to get a 4th dose and those who did not. This weaker methodology leaves the results more susceptible to confounding, less trustworthy. Fifteen percent of Americans over 50 still haven’t even gotten a primary course of vaccine, much less boosters, and with the US about to face a shortage of doses for the first time priority should be given to the unvaccinated and unboosted. Italy is still offering dose 4 only to the immunosuppressed, which at this point makes sense to me and to at least some others, though I would add the very elderly and those with multiple preexisting conditions.
AstraZeneca: Though it’s been dismissed by now in the US and Europe for low efficacy, questionable research, and serious (though rare) side effects, the company is back to defending its cheap and convenient vaccine, saying it’s already saved more than a million lives and will save many millions more in developing countries. Maybe so.
The mRNA derby: Why is Moderna’s vaccine consistently more effective than Pfizer’s? Partly, it is thought, the dose: Moderna’s 100 µg original dose, and even its 50 µg booster, are heftier than Pfizer’s 30 µg. But a recent studyhas revealed another reason: Moderna stimulates parts of the immune system that Pfizer doesn’t, including but not limited to inducing IgA “mucosal” antibodies believed key in preventing infection.
Little kids: Pfizer’s 3 microgram vaccine for under-5’s flunked out – it didn’t even stimulate toddlers’ immune system. A 2-dose cycle of Moderna’s 25 microgram version for children 6 months to 6 years old, on the other hand, works even in the real world. Efficacy was only around 40%, but against Omicron that’s par for the course. No kids developed severe disease, so we can’t say anything about that endpoint.
School-age kids: Parents get widely castigated for not getting their kids vaccinated, giant campaigns are being instituted, and some even propose the shot be added to the obligatory list for attending school. But only 27% of 5-11-year-olds are vaccinated nationally, 45% in vaccine-friendly New York City. Given that those low-dose Pfizer jabs turn out to work not for months but for weeks, I tend to be with those hesitant parents.
Adolescents: Teenagers, unlike kids, seem to remain more than 90% protected – at least against hospitalization for the Delta variant – for close to a year after their second dose. Against Omicron only 40%, in line with results among adults.
Two doses against Omicron: I mentioned a large British study last time but I skipped past what may have been its most important finding: a mere 3 months after your second dose of Pfizer, when you’re still eligible for the Italian Super Green Pass, your protection against Omicron is only 25%.
One dose in survivors: Yet more evidence, this time from Israel, that people who have recovered from COVID-19 need only a single dose of vaccine. Pfizer was 82% effective in preventing reinfection in patients ages 16-64, and 60% in those over 65, whether they received one dose or two – pre-Omicron. I.e. Italy has it right, the US has it wrong.
Omicron specials: One of the plusses of mRNA vaccines was supposed to be the ability to adapt them easily to new variants, and as late as January Pfizer was promising it would have an anti-Omicron vaccine ready to roll in March. Now that deadline has come and gone, and who’s gotten the vaccine? Animals, mainly, and it hasn’t done them much good. Even a tailored Moderna vaccine is flunking out in monkeys and mice. Even worse, the antibody patterns suggest the new vaccines leave the animals less protected against previous strains of the virus. Early human studies are underway from both Pfizer and Moderna, but I suspect it’s back to the drawing board.
Vaccinated/contagious: People with breakthrough infections have a lower infectious viral load than the unvaccinated and clear the virus more rapidly. And researchers in the UK and the Netherlands found people with “breakthrough” infections transmitted the Delta variant to about half as many contacts. But when it comes to household members, who are more intensely exposed, that advantage disappears.
About them chickens…

Currently 31.2 million Americans are uninsured, and that number may swell to 47 million when the Medicaid rolls get slashed due to the end of the state of emergency later this year. Many are theoretically eligible for other forms of insurance, but in practice there are many barriers. As I reluctantly predicted in my last post, the refusal of Congress to fund the battle against COVID-19, for which Democrats are as responsible as Republicans, means those 47 million will likely have to pay for services that had been free: each test will set them back $125-$195, each vaccine dose at least $40, and if they get sick they’ll be liable for treatment costs. Already black or impoverished Americans are being hospitalized at twice the national rate, even before cutbacks kick in. Insured Americans will suffer too, since supplies of vaccines and treatments will dry up, traditional Medicare will no longer cover telemedicine, and the ability to detect and protect against new variants will be damaged. The criminal American health system – or should I say death system – strikes again. When the hell is the US going to join the rest of the civilized world and offer health care to everybody?
The state of the States
New CDC data suggest that 43% of Americans, including more than half of children under 18, have already been exposed to SARS-CoV-2, doubling the official number of cases. But those figures come from analyses of blood samples drawn during January for other reasons – a questionable methodology, given that people who are getting blood tests are older and sicker than the general population, and may also have differing risks of exposure to COVID-19. Only age could be adjusted for statistically. Alas, these findings can and will be misinterpreted as meaning that 43% of Americans not only have had COVID-19 but have permanent future protection due to natural immunity.
The lenient new CDC guidelines continue to be hotly debated, partly related to the agency’s gradual corruption by economic and business interests, with immunosuppressed justifiably fearful. The Italian Medical Association strongly recommends everybody keep wearing masks inside public spaces even if the government goes through with dropping the requirement at the end of April.
In addition to thinking the US should return to normal, Leana Wen thinks an Omicron BA.2 surge is coming but we shouldn’t worry. Her reasoning is that most Americans are protected from severe disease and death by recent infections or boosters. But protection from milder forms is less, and my mantra – shared by experts such as Danny Altmann – is as always, “What about long COVID?”
Another fellow-Cassandra is Tom Frieden, Director of the CDC in better days, who particularly emphasizes how urgent it is get more shots into American arms given that a mind-boggling 60% of Americans are not up-to-date with their vaccines and therefore at particularly high risk for severe disease and death.
Here's that good piece of hers.
Long COVID news (this Times article and this Al Jazeera video recommended)
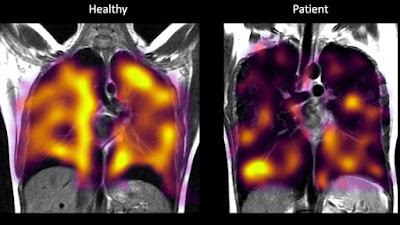 |
| Xenon gas MRIs showing poor oxygen transport in long COVID |
Prevalence
Half the patients with mild-moderate COVID-19 still aren’t well after 6 months, and sicker ones do even worse: a yearafter being discharged from the ICU 74% had persistent symptoms, and only 42% of those previously working full-time were back on the job. And countless outpatients have “medium COVID” that drags on for many weeks.
Most long COVID patients simply continue with the same symptoms they had to start with, but new organ damage can also appear. In one study, COVID-19 survivors were more likely than controls to develop atrial fibrillation, heart failure, heart attacks, and strokes. Other late consequences can include diabetes, kidney damage, hypertension, and dementia.
Fortunately fewer than 1% of pediatric COVID-19 patients develop long COVID and those who do, mostly adolescents, are usually OK by 5 months.
One international research group that followed 309 COVID-19 patients found that 4 patient characteristics predicted prolonged symptoms: type 2 diabetes, high blood levels of SARS-CoV-2, Barr-Epstein virus reactivation, and autoantibodies. Swiss researchers reported 4 different predictors: more symptoms, advanced age, history of asthma, and low levels of IgG3 and IgM antibodies. What to make of the discrepancies?
Diagnosis
“Brain fog” has been considered purely subjective, but that is changing. In-depth neurocognitive testing reveals that even young people with no complaints often have impaired memory and concentration 6 months after mild COVID-19. Structural brain changes have been documented after recovery, impaired brain metabolism demonstrated by 18F-FDG PET scans in patients with cognitive difficulties, and inflammatory markers found in patients’ cerebrospinal fluid.
Many long COVID patients have shortness of breath despite normal x-rays, CT scans, and pulmonary function tests. But one small study from Oxford University documented ineffective oxygen transfer by having patients inhale xenon gas while inside the MRI machine. Another very interesting study, using an invasive form of exercise stress testing, showed that patients who were still short of breath a year after mild COVID-19 had normal oxygen levels in the blood but poor delivery of that oxygen to tissues.
Etiology and treatment
Live SARS-CoV-2 virus may persist in long COVID, as per a Spanish study finding high levels of immune cells with antiviral properties. Only one of their 30 subjects had detectable virus in his blood, but the authors hypothesize that virus persists in bodily tissues, continuing to overstimulate the immune system. Nine of their patients had preexisting autoimmune diseases such as rheumatoid arthritis or psoriasis, suggesting an underlying hyperimmune tendency.
I’d like to see a placebo-controlled trial of antiviral drugs for long COVID. But remdesivir is currently in short supply in both Europe and the USA, and Paxlovid is practically impossible to obtain even for patients supposedly eligible, so no such trial is likely to happen soon. And it’s possible that fragments of viral RNA are what’s stimulating the immune system, not whole viruses that would be susceptible to antivirals.
A controlled study in non-human primates has shown that even relatively mild COVID-19 can infect cerebral blood vessels, bringing inflammation and hemorrhaging, with impaired blood flow reminiscent of the brain scans of long COVID patients with “brain fog.”
Many long COVID symptoms likely reflect poor tissue oxygenation, whether because of clots clogging the arteries or inefficient extraction of oxygen from the blood (possibly with a role for mitochondrial dysfunction). So concentrated forms of oxygen might be therapeutic. Hyperbaric oxygen seemed in fact to help the core symptoms of fatigue and brain fog in one pilot study from the UK, with some patients finding it transformative. This approach is undergoing controlled trials in California, targetting pulmonary symptoms, and in Sweden, targetting fatigue and cognition.
But even if hyperbaric oxygen helps symptoms, it will remain a stopgap unless we attack the root cause, perhaps using anticoagulants to dissolve microclots. Following promising South African data, a large-scale study, STIMULATE-ISP, is going forward in the UK: this consortium will enroll 4,500 long COVID patients, with 1500 receiving the anticoagulant rivaroxaban. I can’t wait to see their results.
A different approach to treating microclots is to filter them out of the circulation using apheresis. One center in Germany has tried this complex and costly method on more than 100 long COVID patients, including a physician who says it cured him – in combination, though, with cheap(ish) and simple anticoagulants.
Farther-out treatments include non-invasive electrical brain stimulation, claimed to have cleared the brain fog of onelong COVID patient, and – undergoing controlled trials –PureTech’s LYT-100 (deupirfenidone) for respiratory symptoms, acupuncture for fatigue, Roche’s Pirfenidone for lung fibrosis, an antidepressant for brain fog, and Resolve Therapeutics’s RSLV-132 for fatigue and brain fog. Also cannabis, the opioid blocker naltrexone, the cholesterol drug atorvastatin, and a whole range of dietary supplements.
Then there’s the IncellDX company, which has already gotten 14,000 long COVID patients to shell out thousands of dollars for atorvastatin and the AIDS drug maraviroc. Its bona fides have been sharply questioned in an investigatory piece in Mother Jones, noting that its founder and CEO, Dr. Bruce Patterson, has been associated with the notorious Front Line COVID-19 Critical Care Alliance, and that he used to promote leronlimab, a failed COVID-19 treatmentwhose publicity earned its company an unusual public reprimand from the FDA. IncellDX now offers its package not only to “chronic Lyme disease” and “myalgic encephalomyelitis” patients but also, ominously, to people who believe COVID-19 vaccines made them chronically ill.
How bad is bad?
The best measure of the human toll of the COVID-19 pandemic is excess mortality, the number of total deaths over what would be predicted from earlier years. For countries with reliable all-cause death records, such as the US and Italy, that calculation is easy (the excess is about 20% in both, of which 90% is due directly to COVID-19). But in low- and middle-income countries many deaths go unreported, and the wish to downplay COVID-19 has increased that proportion. A giant international group of researchers examined the real human costs of the pandemic and concluded that the true pandemic death toll is 18.2 million, triple the official statistic. As you can see from the map, the worst-off countries are in Latin America, southern Africa, and Eastern Europe.
Leak vs. leap
 |
| The Huanan Market |
In case anyone still thinks SARS-CoV-2 leaked from a laboratory, the evidence that it was instead passed from animals to humans at Wuhan’s Huanan Seafood Market is increasingly solid – see summaries in the New York Times, Forbes, and Nature.
American mishegos
 |
| Joseph Ladapo with Ron DeSantis |
• Florida governor DeSantis gets the Pandemic Politician booby prize. He’s still refusing to enforce the federal vaccine mandate for healthcare workers after it was upheld by the Supreme Court, leaving Florida hospitals between a rock and a hard place. And the latest antic of Joseph Ladapo, they guy he hired as Florida’s top physician, is telling parents not to vaccinate their kids?
• Tennessee Republican lawmakers are not far behind. Last September their Board of Medical Examiners declared that doctors spreading COVID-19 misinformation – vaccines contain microchips, etc. – could jeopardize their medical license. State lawmakers promptly threatened to disband the Board, and in December the Board caved. They did eventually repost a wishy-washy version, but zero Tennessee docs have faced disciplinary action.
• An Oklahoma City hospital had to close down a COVID-19 ICU because of online threats accusing doctors of making patients receive “Fauci's death protocol” and being “Wicked Marxist” who “murder God's people.” One Facebook post provided a physician’s home address, superimposing the word MURDERER over his photograph.
• Should novaxxers be allowed get organ transplants? For me that’s a no-brainer, the sacrifice someone made to give that organ is in vain if the organ is destroyed by COVID-19. Many major institutions agree, but I’m shocked to see a majority do not….
International mishegos
 |
| A pro-Djokovic demonstration in Serbia |
When Australia barred entry to tennis superstar and proud novaxxer Novak Djokovic early this year the dominant global reaction was outrage at his arrogance, but in Djokovic’s native Serbia, where only 48% of the population has had even one vaccine dose, he’s a national hero (but, hey, Serbia beats Bulgaria’s 30%!).
I mentioned last time that vaccine coverage of the elderly was low in China. But I didn’t realize just how low until I read in a Hong Kong manuscript that as of January, “two-dose vaccine coverage had only reached 46% in older adults 70-79 years of age and 18% in those aged 80 years.” No wonder they’ve had to lock down Hong Kong and Shanghai.
Italy gave fair warning back in January that all novaxxers over age 50 would be punished with a fine: €100 ($110). Now 2 million notices are in the mail. That’ll learn ‘em!
English mishegos
Human challenge studies: Who knew? The Brits began quietly infecting unvaccinated, non-immune people with wild-strain SARS-CoV-2 six months ago. Of 36 young healthy volunteers who had a very low dose of virus shot into their nose, 18 were successfully infected and 16 became ill after 2-4 days. Contrary to the researchers’ early promises, just a few were given remdesivir, the only antiviral available at the time. No volunteers became severely ill but 7 became feverish, many had muscle aches and fatigue, and 12 lost their sense of smell, some for as long as 6 months. Subjects were infectious by 2 days after inoculation and remained so for up to 12 days. CNN generously titled its article, “First human challenge study of Covid-19 yields valuable insights about how we get sick.” What valuable insights exactly? None that I could see.
Head counts: The AstraZeneca vaccine is not the only aspect of the UK’s epidemic surrounded by weirdness and lies. It also fudges its death statistics: “A death can only be recorded as a COVID-19 death where a positive test was received if this positive test was received within 28 days of their death.” They devised this brilliant trick in August 2020, thereby slashing their official death toll by 12% in one fell swoop. These shenanigans are medically absurd – COVID-19 patients notoriously can hang on life support for weeks, even months.
In the trash: But the greatest mishegos of all is Boris Johnson scrapping all pandemic restrictions in England on February 24th, including self-isolation. He did get blowback, and the UK government’s scientific advisory board predicted large increases in community transmission. In fact, the BA.2 subvariant arrived in time to send the 7-day average of new cases in the UK from 37,214 on February 27th to 123,451 on March 24th before falling off slightly. Hospitalized cases rose from 10,561 to 18,809 [update on March 30th). And hundreds of flights have been cancelled because crews are out with COVID-19 – as Eric Ding says, wasn’t “let it rip” supposed to be good for the economy?
Old conspiracy theories never die, they don’t even fade away
Think the hoax theory died out long ago? So did I, but we’re wrong
• Headline from The Geller Report: “MIT Scientist Warns Parents NOT TO GIVE CHILDREN Vaccine, Could Cause ‘Crippling’ Neurodegenerative Disease In Young People.” Yes, Stephanie Seneff is really an MIT computer scientist. She’s also convinced COVID-19 vaccines cause mad cow disease.
• Then there’s the osteopath who calls COVID-19 vaccines deadly bioweapons or “depopulation vaccines,” saying depopulation would start by last August. Haven’t you noticed people disappearing?






















